
ベストサプリメント賞、5年連続受賞!生酵素サプリ

酵素はさまざまなスタイルでサプリメントに取り入れられています。
ダイエットサポートや毎日のハリ、若々しい健康的な毎日のサポートに、生酵素のサプリメントが注目を集めています。
プロのアスリートにも愛用している人が多く、プロ野球選手の工藤公康さんはそのひとりです。世界中10か国以上で400万個以上の売り上げがあることでも、人気のほどがうかがえます。
生酵素は、厳選された100パーセント国産の植物材料、季節ごとに旬の野菜や果物をたっぷり投入して作っています。
発酵させて熟成させている間も、一切加熱処理をしないので、乳酸菌、アミノ酸、有機酸といった有効成分が壊れずに生きています。
生きた有効成分を凝縮したカプセルサプリメントです。
生のエキスをカプセルに閉じ込めているから、味が気にならない、持ち歩きに便利、常温でも保存がきくといったメリットがあります。
酵素ダイエットは、食事の回数を減らし、食事の代わりにサプリメントを取るという方法です。適度な運動も組み合わせて行います。
朝ごはんを食べる時間がないから抜いたままにしないで、その分酵素サプリメントを飲んで、ダイエット中の栄養バランスの偏りをサポート。
オーエムエックス生酵素だからダイレクトに効く!毎日の元気に

酵素ドリンクの独特の味や、甘いドリンクのカロリーが気になる人は、カプセルタイプのサプリメントも便利です。
朝すっきり起きられない人、食習慣や生活習慣が不規則な人、ダイエットはしたいけれど、体調が悪くなったり、スキンコンディションに問題が出たりするのが気がかりという人には、酵素サプリメントがおすすめです。
サプリメントは一定期間継続してとることで良さが実感できます。生酵素のサプリメントも、数か月ためして体調にどのような変化が見られるか、実感してみたいですよね。
ファッション誌を中心に、雑誌やメディアでも好評です。発酵食品は日本の食文化の中ではとても大きな部分を占めます。
日本人の健康を支えてきた発酵食品ですが、食の西洋化が進み、毎食発酵食品を食べるという人も減ってきています。
サプリメントなら、定期的に決まった量の酵素を摂取することができて効率的です。
天然由来の栄養素が凝縮されています。

「もう若くないのかな・・・」
ちょっと前だったら、朝までみんなと飲んでいてもそのまま仕事ができていたのに、最近ではてっぺんまわるはおろか11時ぐらいにはお酒もだいぶまわって眠くなっちゃうような状況で・・・。
お酒を飲んでいないときだって、次の日の朝にカラダがだるくて重くて、疲れが残ってる感じが!
だからやる気も出ないしモチベーションも上がらなくって!!
まだまだ頑張らないといけないのに、気持ちは昔のままでもカラダが最近ついてこなくなっちゃって・・・。
あなたも最近こんなカラダの変化、気になっていませんか。
そしてその体調の変化を年齢のせいにしていないでしょうか?!
年齢を重ねることでおきるこのような
- スタミナ不足
- 朝スッキリ起きられない
- やる気も出ない
といった変化は、もしかしたら「酵素不足」かもしれません。
「酵素がなくなった時に生物は死を迎える」
と言われるほど、酵素は大切な存在。
酵素と聞くと「消化」というイメージがありませんか?
でも実際にはカラダを動かすにも、物事を考えるのにも、ありとあらゆる行動に酵素の存在は欠かせません。
年齢を重ねることで感じるカラダの不調は体内で生み出される酵素が減少していき、酵素不足の状況が引き起こしている可能性は低くありません。
年齢を重ねるごとに減少していく酵素は生野菜や生フルーツ、お刺身などの生肉、ヨーグルトや納豆といった発酵食品から補給することが可能ですが、私たちの食生活の多くは酵素を補うどころか浪費する食事となっているのが現状です。
総菜コーナーで揚げ物、手軽な加工食品・・・etc.
これらの普段口にする食事では酵素が含まれていないどころか、食品添加物などで余計に酵素を浪費するような食事になってしまっていて、これが年齢による減少とともに酵素不足に拍車をかけ、あなたの健康を脅かし、老化を促進している大きな原因の一つと考えられます。
でも、なかなか“酵素満点”の食事は大変!
では減っていく一方の酵素を補うにはどうすればいいかというと・・・「サプリメント」が一番手軽でおススメ!!
生きた酵素だから腸までしっかり届く!
でも、注意点が1つあります。
それは生きている酵素を補給できなければまったく意味がないということ!
酵素は熱に弱く、火を通した食材ではほとんどが壊れてしまっています。
サプリメントも製造工程で熱がかかってしまっているものが多く、酵素を補うという目的を果たせないものが数多く存在しているのが実情・・・。
そのような状況の中、酵素をしっかりと補給することができる「生酵素」ともいうべきサプリメントがあります^^
そのサプリメントの名は・・・【オーエムエックス】!
野菜や果物、野草など様々な素材に一切火を加えずに乳酸菌の発酵でドロドロにし、それをカプセルに閉じ込めた【オーエムエックス】。
酵素ドリンクでは独特な風味で飲みにくいなんていうことも少なくありませんが、カプセルタイプなら味も気にせず確実にあなたのカラダに酵素を補給することができます!
「年齢のせいかな・・・?」
そう思ったなら、酵素不足を疑ってみてはいかがでしょうか^^
オーエムエックスの生酵素は、健やかな毎日をサポートしてくれます

睡眠時間はたっぷり取れているはずなのに、朝起きるのが辛くなった、疲れが取れていないように感じている現代人は、案外多いようです。
健康に気を使いたいと思ってはいても、身体にいいこと程なかなか難しく、身体のためにとがんばってみても、いつも三日坊主で終わってしまうのではないでしょうか。
身体のためにとがんばることはとても良いことですが、それがストレスになってしまっては本末転倒です。
健康に欠かせない栄養素がぎゅっと凝縮されたオーエムエックスのカプセルなら、がんばらなくても続けられます。
黒いカプセルの中身は、生の酵素です。
酵素という言葉は聞いたことがあるという方もいらっしゃるでしょう。
最近、数々のメディアでも取り上げられている、注目の栄養素です。
酵素は、人間が生きていく上で欠かすことはできません。
ですので、酵素は体内で作り出すことが出来るのですが、年齢によりその分泌量は減っていってしまいます。
酵素が不足すると、食べた物を消化するのに時間がかかったり、お酒がなかなか抜けなかったり、疲れが取れにくくなってしまったりというような不都合が起こってしまうのです。
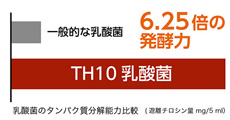
6.25倍のパワーを誇るTH10乳酸菌で発酵
そんな大切な酵素は、果物や野菜などに多く含まれています。
しかし、酵素は熱に大変弱いため、加熱調理されたものからの酵素の摂取は難しいでしょう。
だからこそ、オーエムエックスの生酵素は、その名の通り、生にこだわっています。
全て国産の、選び抜かれた野菜や果物を使用し、一切の加熱処理を行なわずに、乳酸菌の発酵の力で酵素の素となるアミノ酸や有機酸を作り出すのです。
そして、日本の春夏秋冬の温度変化を利用して熟成させるので、酵素をはじめとした栄養素の全てを、生のままで凝縮させることが可能となりました。
更に、カプセルに充填する際も、高温は加えないと言った徹底ぶりです。
酵素を摂取する方法としては、ドリンクタイプが一番吸収が良いとされていますが、酵素が濃いものほど、独特の飲みにくい風味がありました。
それをごまかすために、ほかのジュースで割って飲む方もおられるようですが、そのジュースに糖分が入っていると、せっかく取り入れた酵素がジュースの糖分を分解するために使われてしまいます。
しかしカプセルなら、お水で飲み込むだけですので、酵素の風味が苦手な方でも無理なく続けることができます。
オーエムエックスの生にこだわったカプセルは、吸収が良い分、効果が現れるのも早いでしょう。
オーエムエックス口コミ・評判
暮らしのお役立ちサイト
アイドラッグ 富士登山レンタル富士山の下山の途中で返却が可能で登山に行くついでにも借りることができます。
mixhost ログイン ビーナスベッド
お洒落なデザインの家具が豊富に揃っているライフスタイルに合わせた家具をご提案。
トーカ堂
使途自由なキャッシングプランで借り換えも可能な消費者キャッシングのアローになります。